
Demand in general practice is high for the time of year, not just in the media but in the data. It may result from a combination of changes coming out of lockdown, delays in secondary care or easier access, but we don’t have convincing evidence of which is most significant.
The question of what to do about it can’t be separated from the cause, as a wrong diagnosis and resulting wrong solution may make the situation worse. Some have speculated that easier access online is driving up demand, which sounds logical although we saw no evidence of that pre-covid. Nevertheless, if better access has uncovered unmet need that was there all along, what should be done?
One suggestion is to reduce the hours in which online access is available, and Steve Black has taken a look at the outcomes in terms of total demand as a % of list size, since the start of 2021. In the first example, online is available 24/7, although patients are told if they are out of hours to expect a reply on the next working day. Grey bars represent availability, and the red line shows total demand.
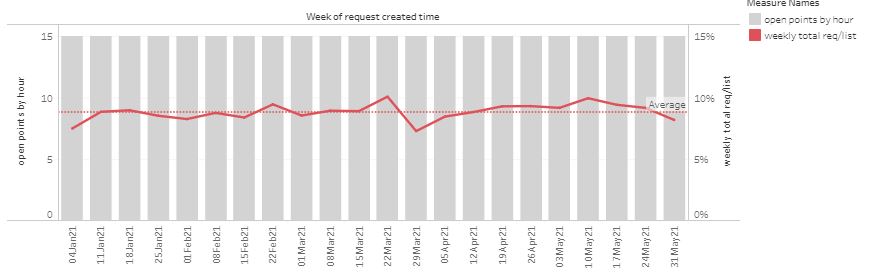
“Open point” is a score based on the period when patient requests can be submitted, weighted towards normal contracted hours. The red line is total demand (online and telephone requests) as a % of list size, per week.
In the following example, opening hours were cut in response to perceived high demand.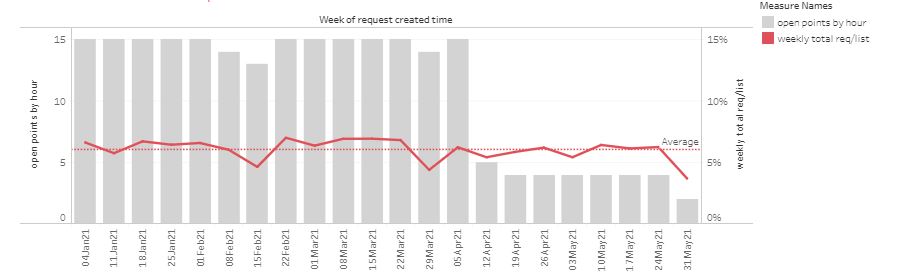
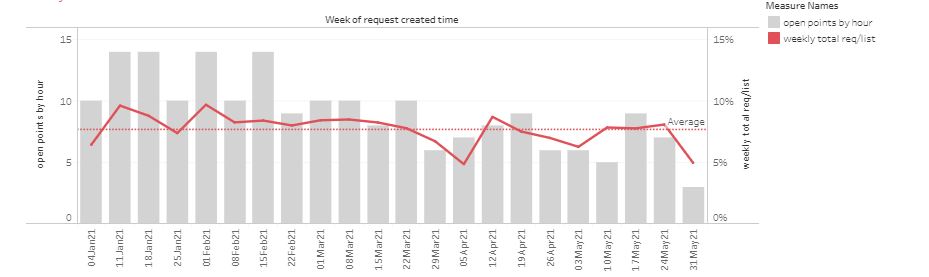
Another practice has made multiple changes in an attempt control demand, sometimes significantly reducing availability even in-hours.
 Overall, changing opening hours has had little effect on demand. However, as a patient there is a loss of service as they cannot be so sure they can submit a request online when they want to. Constantly changing the time the system is turned off risks patients losing trust in the online route, driving more demand through the telephone route which is less efficient to manage.
Overall, changing opening hours has had little effect on demand. However, as a patient there is a loss of service as they cannot be so sure they can submit a request online when they want to. Constantly changing the time the system is turned off risks patients losing trust in the online route, driving more demand through the telephone route which is less efficient to manage.
Taken to the limit, turning off online access completely would return to purely telephone access, with none of the flexibility for both patients and staff to use the efficiency of messaging and workflow.
Are there other advantages in cutting hours? Some take the view that they feel more in control if they know that no new requests can arrive after a certain time. Others turn off access at weekends, on the basis that some issues may have self limited by Monday, or they don’t want to see requests stored from the weekend, adding to a busy Monday.
Our usual advice to practices has been to keep online access open all the time, both in-hours and for OOH times when the message to patients sets a different expectation. However, we are clear that practices may turn off access themselves, either routinely or ad-hoc for example in the case of staff absence.
Based on the new data, we would suggest:
1. Reducing access hours has very little effect on total demand.
2. Practices may choose to limit hours, and it’s better to have consistent times so patients can be confident that online is open.
3. Whatever the decision, it should be up to the practice to determine access hours, and easily controlled by practice staff.






[…] Whilst Tower Family Healthcare has temporarily closed AMGP requests due to the effects of Covid-19, pressure and demand, Harry Longman continues to champion that leaving the system on would not dramatically increase this demand. He uses examples of practices like Dr Arnott’s and Dr Sangha’s alongside three example graphs. […]